

Purpose
Reporting of total reference air-kerma (TRAK) as a brachytherapy treatment parameter is recommended by the ICRU Report 89 [1]. TRAK is defined as the integral of reference air-kerma rate over the treatment duration, and summed for all source dwells (expressed in units, such as cGy at 1-meter reference distance). Historically, TRAK is related to the milligram-hour radium concept (radium mass × treatment time), and therefore represents intensity of treatment. Also, TRAK does not take into consideration geometry of brachytherapy application, and is considered an unambiguous physical quantity. While TRAK does not portray the shape of target volume treated nor predict dose distribution for a given application; however, dose to any point or volume is directly proportional to TRAK value [1]. In intracavitary brachytherapy, TRAK has been shown to correlate with volume enclosed by isodose surface (ISV). Accordingly, predictive mathematical expressions relating volume enclosed by isodose to TRAK and dose are suggested in literature [2-7].
In this study, we aimed to relate TRAK to volume enclosed by the prescription isodose surface (ISVRef) in a single-channel vaginal cylinder (VC) high-dose-rate (HDR) brachytherapy. Since VC brachytherapy represents one of the most widely utilized gynecological brachytherapy applications [8], we felt it would be interesting to obtain TRAK-irradiated volume relationship and compare it to the published TRAK-volume relationship for intracavitary brachytherapy.
Material and methods
Brachytherapy treatment plans of 175 patients treated for gynecological cancer at our institution with iridium-192 (192Ir) HDR brachytherapy, using single-channel VC applicator (Elekta AB, Stockholm, Sweden), were retrospectively reviewed. VC size distribution was 20 mm (n = 4), 25 mm (n = 12), 30 mm (n = 52), 35 mm (n = 104), and 40 mm (n = 3). Treatment length ranged from 30 mm to 90 mm (median, 50 mm). Brachytherapy dose (DoseRef) of 5 Gy per fraction was prescribed at 5 mm depth from cylinder’s surface. A commercial treatment planning system based on the AAPM TG-43 dose calculation formalism was utilized for dose planning and optimization (Oncentra; Elekta AB, Stockholm, Sweden). Source dwell times in each case were optimized using dose-point optimization, with dose points described laterally to the cylinder surface and superiorly at the cylinder dome. Source position separation (step-size) applied in treatment plans ranged from 2 mm to 5 mm. Previously, with our HDR microSelectron v2 afterloader (Nucletron), the source step-size in increments of 2.5 mm was possible, whereas in our current Flexitron HDR (Elekta) afterloader, source position separations within 1 mm increments are possible. Either a 2.5 mm or 5 mm source step-size was applied in planning with microSelectron-HDR v2 afterloader, and a 2 mm or 3 mm source step-size was utilized with Flexitron HDR afterloader, which was achieved by activating every 2nd or 3rd dwell position. In general, finer step-sizes (2 mm or 3 mm) were used for shorter treatment lengths (≤ 50 mm), and coarser step-size of 5 mm was applied in longer cylinder treatment lengths (≥ 50 mm). Patients were treated either with a microSelectron-HDR v2 or a Flexitron HDR treatment unit.
From each patient’s brachytherapy treatment plan, the following parameters were extracted: TRAK (cGy at 1 meter) representing the fractional total reference air-kerma of brachytherapy treatment, planned source strength (in Ci), total treatment time (in seconds), and isodose surface volume corresponding to prescription isodose (ISVRef in cm3) from a dose-volume histogram. Additionally, the volume of vaginal cylinder included in ISVRef was calculated by contouring the vaginal cylinder length enclosed by the prescription isodose and obtaining the corresponding volume. In each case, real irradiated vaginal tissue volume (VVT) with prescription isodose was then calculated by subtracting the cylinder volume enclosed by the prescription isodose from ISVRef. For the purpose of the study, in each case, the planned total treatment was normalized to the time required for a 10 Ci apparent activity 192Ir source. Data were analyzed using basic statistics and graphing tools (Microsoft Excel).
Results
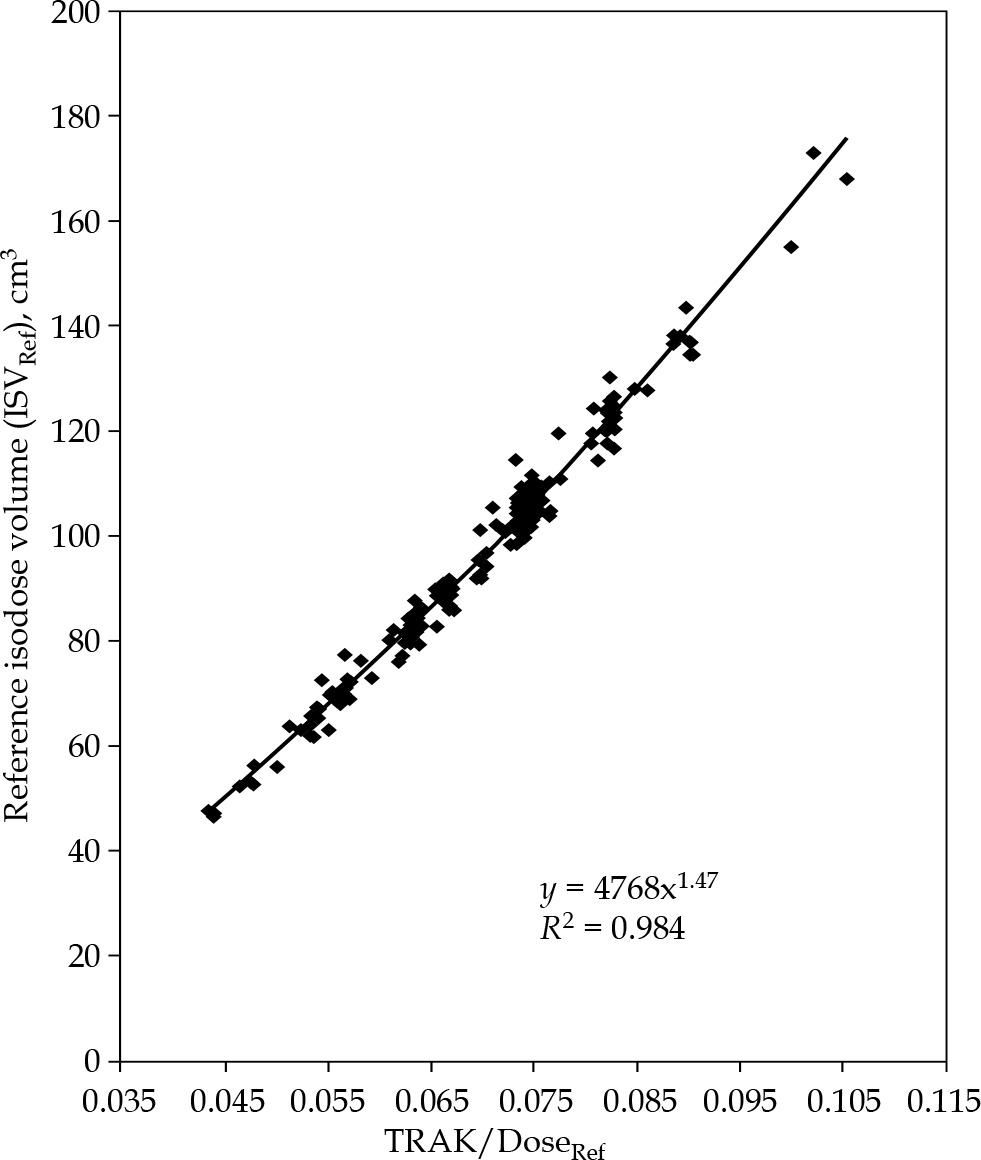
TRAK vs. reference isodose surface volume
A scatter plot of (TRAK/DoseRef) vs. ISVRef is presented in Figure 1. TRAK exhibited a relationship with ISVRef, which was best described by a power-law type equation (R2 = 0.984):
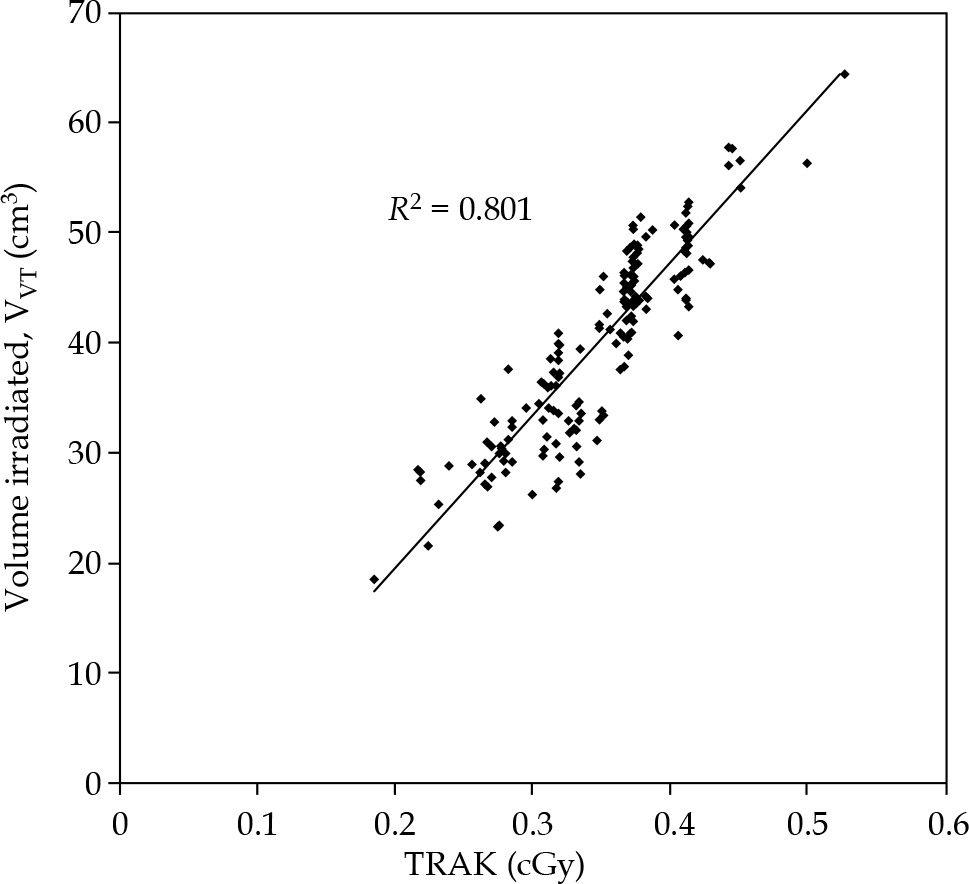
TRAK vs. vaginal tissue irradiated volume
A scatter plot of TRAK vs. VVT is presented in Figure 2. TRAK exhibited a relationship with VVT, which was best described by a linear equation (R2 = 0.801):
TRAK vs. treatment time
A scatter plot of TRAK vs. total treatment time is presented in Figure 3. TRAK related to treatment time was shown via a relation:
Fig. 3
A scatterplot of TRAK vs. total planned treatment time for 175 vaginal cylinder brachytherapy cases. TRAK – total reference air-kerma (cGy), total treatment time in seconds for a 10 Ci apparent activity of 192Ir source
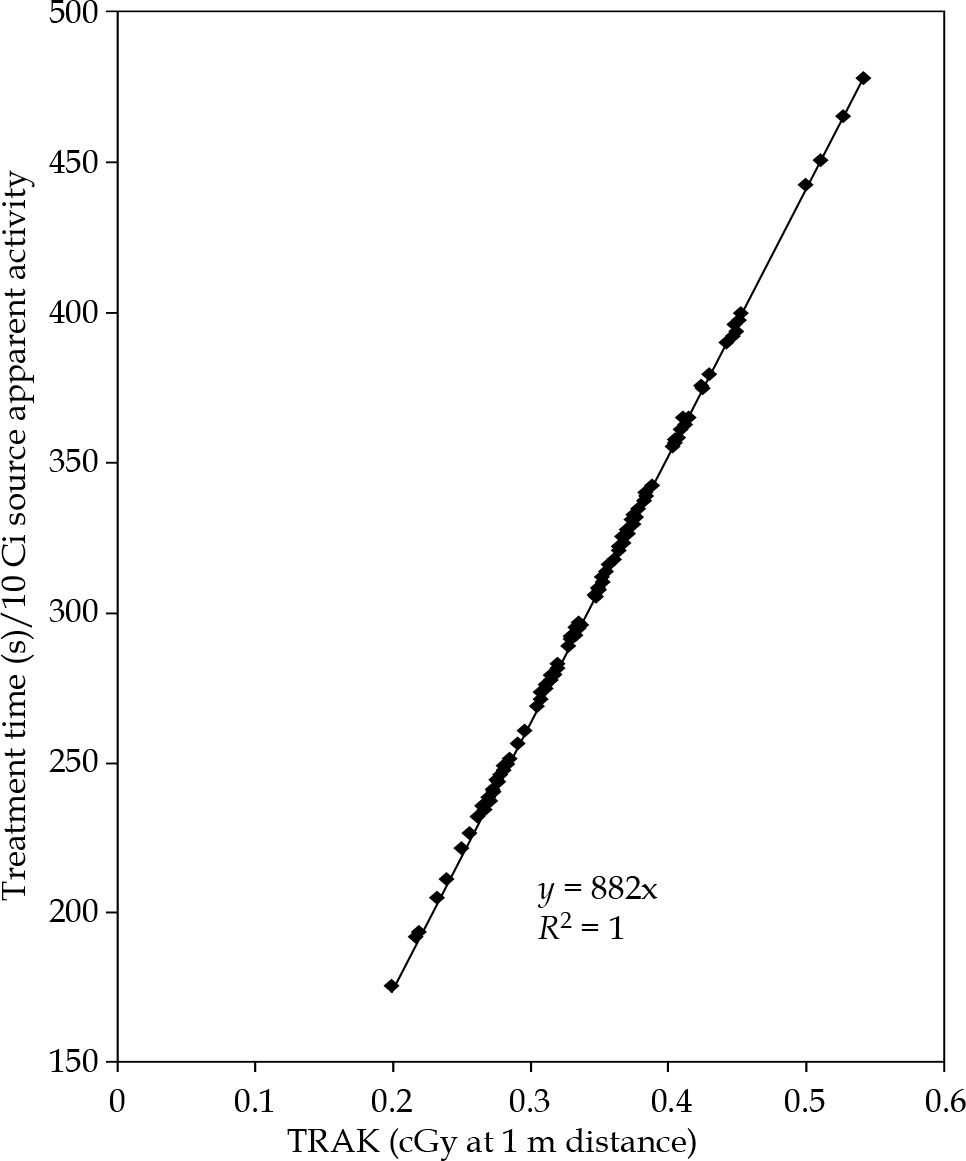
where 882 is (1/air-kerma strength) for a 10-Ci apparent activity 192Ir source.
Discussion
The power-law relationship between TRAK and the volume enclosed by the prescription isodose surface based on our study data (Eq. 1) yielded a predictive equation, which is similar to the one proposed by Wilkinson and Ramachandran [2]. In their study, the authors proposed that the spherical volume covered by any dose level can be calculated by the expression: V (cm3) = 4965 (TRAK/DRef)3/2, presuming that the total activity is concentrated into a point-source and distance following inverse square law for dose gradient. While the ICRU 89 Report [1] recommends reporting of TRAK as a parameter, ISVs in cervix brachytherapy could be utilized for reporting treatment intensity and for comparing treatments across fractionation schedules [6, 9]. In VC brachytherapy, the irradiated surface volume at the prescription dose level also includes the volume of VC utilized for the patient, and does not strictly corresponds to the irradiated tissue volume. It is not a standard universal practice in clinical VC brachytherapy to routinely adapt contouring of target volume during treatment planning. This is mainly due to differences between practitioners on where the dose is prescribed (at surface vs. at depth), and also because of differences in dose optimization methods utilized [8, 10]. In our opinion, this limits the clinical utility of reporting ISVRef in VC brachytherapy. Interestingly, in our study, we observed that TRAK data correlates linearly with the volume of vaginal tissue covered by the prescription dose (Figure 2; Eq. 2). Various studies on VC brachytherapy have shown correlations between total dose, dose per fraction, vaginal length treated, and vaginal late toxicity [8, 11]. Since vaginal length treated is directly related to volume of vaginal tissue irradiated, one could presume that by reporting TRAK as a treatment intensity parameter, TRAK will play a vital role in studies related to treatment toxicity in VC brachytherapy.
The relationship between TRAK and the total treatment time presented in Eq. 3 is a result of definition of TRAK [12]. This relationship could be utilized as a hand calculation method to quickly verify planned treatment time, knowing the value of TRAK from treatment plan in any HDR brachytherapy application. This method, by itself, does not exactly constitute an independent second-check of the treatment time since the TRAK value input is taken from the treatment plan. However, it does add a value as an additional quick overall check of planned treatment time for a given TRAK value by a physician or a physicist [13]. As presumed in the previous statement, a thorough independent check of the treatment plan by a secondary check method (as required in published QA guidelines) was performed, and our proposed treatment time check only serves as an additional plan QA tool prior to treatment.
Additionally, TRAK parameter could be utilized as a secondary plan quality check parameter to establish a range of optimal TRAK values for specific VC applicator size that could be derived based on individual institutional dose prescription and optimization practices. In our study, the average TRAK values for the cylinder diameters utilized were: 0.23 (size 20 mm), 0.27 (size 25 mm), 0.32 (size 30 mm), 0.38 (size 35 mm), and 0.46 (size 40 mm). Ideally, one would expect a fixed value of TRAK for a given VC size, dose, length, and fixed depth of prescription. However, differences in TRAK values exist depending on the method used for dose optimization, such as lateral dose points only or lateral dose points plus accounting for curvature of cylinder dome. These differences could result in different volumes irradiated by the prescription dose [10].
Conclusions
The correlation of TRAK to the total volume encompassed by the prescription dose surface in a single-channel vaginal cylinder brachytherapy yields a useful predictive equation, but restrictive in application due to differences in dose optimization schemes, implemented for vaginal cylinder HDR brachytherapy treatment that vary in clinical practice. However, the linear correlation observed between TRAK and the volume of vaginal tissue irradiated, could be of clinical interest in treatment toxicity-related studies. The TRAK treatment time relationship enables quick verification of planned treatment time by knowing TRAK in any HDR brachytherapy application.